
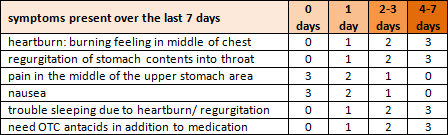
Heartburn – an uncomfortable burning sensation in the chest or throat due to stomach acid in the esophagus – affects at least 20% of Americans on a regular basis. Frequent heartburn is known as gastroesophageal reflux disease (GERD). A score of 8 points or more on the following questionnaire indicates at least an 80% likelihood that GERD is the correct diagnosis.
what causes gastroesophageal reflux?
The stomach normally sits just below the diaphragm, positioned so the hiatus (opening) of the diaphragm reinforces the LES (lower esophageal sphincter), a muscular ring meant to keep the acidic environment of the stomach separate from the esophagus.
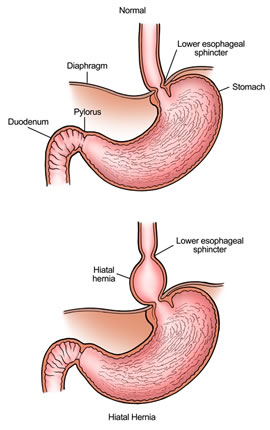
The LES should always remain closed except to allow food into the stomach during meals. Failure of the LES is the most important factor in GERD. Possible reasons for a weak LES include
- hiatal hernia, where part of the stomach is pushed above the opening in the diaphragm (refer to diagram)
- obesity due to increased pressure on the stomach
- stress and sympathetic dominance
- intestinal malabsorption, including lactose intolerance, which increases gastric distention
- eating fried fatty foods and other “crap”:
C = coffee, cigarettes, chocolate, corticosteroids
R = refined sugars
A = acidic foods, alcohol, allergens (food sensitivities)
P = pop (soda), peppermint, packing in food (overeating)
Once the LES is not functioning properly, acid from the stomach and sometimes even bile salts from the duodenum (small intestine) can splash back up into the esophagus; this is the definition of “reflux”. Such chemical irritation causes inflammation and oxidative damage; repeated exposure to duodenal and gastric juice eventually leads to cellular changes in the esophagus called Barrett’s metaplasia, which is a precancerous condition known to increase the risk of dysplasia and esophageal adenocarcinoma (cancer).
proton pump inhibitors
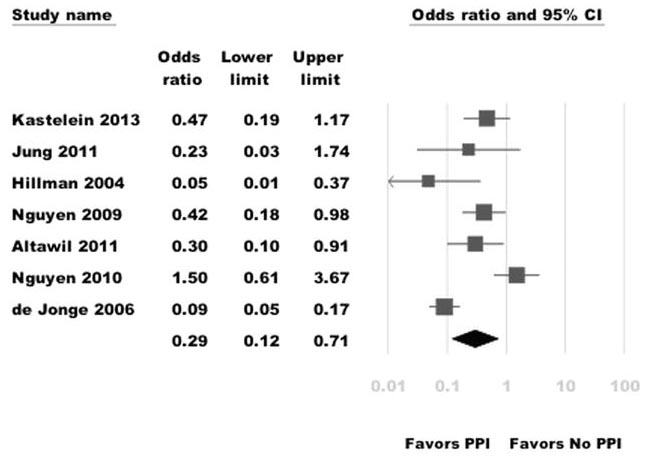
The gold standard in conventional treatment of gastroesophageal reflux are the proton pump inhibitors (PPI) – omeprazole (Prilosec), esomeprazole (Nexium), pantoprazole (Protonix), and lansoprazole (Prevacid). These drugs work by irreversibly blocking the H+/K+ ATPase “proton pump” of parietal cells in the stomach, preventing the release of hydrochloric acid. The rationale for using these drugs in the treatment of GERD is that decreasing the acid content of the refluxate should prevent damage to esophageal tissue. And in fact there is some convincing evidence that PPI therapy can decrease the risk of esophageal adenocarcinoma, as in this 2014 meta analysis:
However, in the twenty-some years that PPIs have been on the market (and wildly popular, the #2 selling drug with over $6 billion in sales in 2013), 10-40% of patients still experience heartburn.
In addition to noncompliance or patient error such as taking the medicine without regard for mealtime, a commonly cited reason for PPI treatment failure is that only 70% of proton pump enzymes are inhibited by the drug at any time.
In my mind a much more important reason is that proton pump inhibitors actually decrease muscle tone of the LES, perpetuating the original reason for gastroesophageal reflux!
pantoprazole may impair gastric and lower esophageal sphincter muscle tone and thus paradoxically exacerbate esophageal reflux – Welsch et al. 2014
Many PPI non-responders are assumed to have the GERD subtype called “NERD” (non-erosive reflux disease) which may involve factors such as impaired esophageal mucosal barrier function, visceral hypersensitivity, and altered esophageal motility rather than acid.
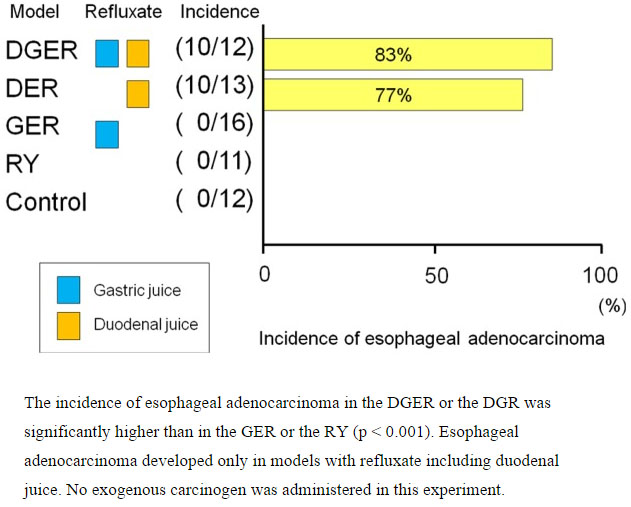
Also consider that 68.7% of nonresponders have bile reflux from the duodenum. Much of the newer research has demonstrated the importance of bile salts in the etiology of heartburn symptoms and pathologic changes in the esophageal mucosa. The following chart shows results from a surgical study performed in rats, where the presence of duodenal juice was the definitive factor in the incidence of esophageal adenocarcinoma:
Clearly, stomach acid is not the only contributing factor to GERD and its symptoms; so perhaps proton pump inhibitors should not be regarded as the only “best” way to manage the issue.
side effects and risks of PPI therapy
There are several major adverse effects caused by proton pump inhibitors. Those discussed below are largely cumulative over time, so the longer the PPI medication is used the greater the risk.
- Altered stomach architecture, which may manifest as rebound acid hypersecretion and/or atrophic gastritis, especially if H. pylori infection is present.
- Increased risk of food allergies due to incomplete digestion of proteins; gastric acid levels determine the activation of gastric pepsin and also the release of pancreatic enzymes.
- Nutrient deficiencies due to malabsorption of several essential vitamins and minerals that require stomach acid, including B12, iron, magnesium, and calcium. Long-term use can contribute to anemia, bone fractures, and functional decline and dementia.
- Dysbiosis due to proliferation of pathogenic yeast and bacteria that normally could not survive the acidic environment of the stomach: Clostridium difficile, Klebsiella, Streptococcus, E. coli, Candida albicans, Enterococcus, Bacteroides vulgatis, among many others. Small intestinal bacterial overgrowth (SIBO) occurs significantly more frequently among long term PPI users (50%) than in patients with IBS (24.5%) or healthy controls (6%).
(Although PPIs are officially indicated for only 4-8 weeks at a time, many people diagnosed with GERD end up taking them for the rest of their lives because acid suppression is diminishing the damaging effects of reflux but not really fixing the problem. True safety data for such long-term treatment are lacking; controlled studies do not extend beyond 12 months. The lifelong PPI trend is particularly disturbing as more and more prescriptions are written for children or babies with colic or reflux, despite the fact that clinical trials reveal that PPI therapy is not effective treatment for these common infant GERD-associated symptoms.)
natural alternatives for treating GERD
Just like the causes and triggers of GERD may be different for each person, there is no one-size-fits-all approach for managing the condition without PPIs. However, here are some highlights of the many things I have successfully used with patients:
- Adjust diet to generally avoid spicy foods, alcohol, carbonated beverages, and other “crap” that triggers heartburn episodes.
- Support the parasympathetic nervous system (our “rest and digest” mode) to help increase muscle tone of the LES: stress management, taking time to sit down and enjoy meals, etc.
- Maintain a healthy weight to minimize external pressure on the stomach; eat smaller meals throughout the day to minimize pressure and distention within the stomach.
- If hiatal hernia is present, find a naturopathic doctor trained in visceral manipulation to readjust the position of your stomach so it sits below the diaphragm again.
- Soothe and protect the esophagus and stomach lining with healing herbs and nutrients if heartburn still occurs. (A Finnish research group recently published a study using hyaluronic acid and chondroitin sulfate for NERD with this same intent).
- Improve digestive function with digestive enzymes and probiotics; also assess for and eradicate any overgrowth of pathogenic microbes.
(additional notes)
Other medical and surgical options exist for treating GERD, of course, including H2 blockers, prokinetic agents, various methods of fundoplication, and a fascinating new procedure involving magnetic sphincter augmentation. These are beyond the scope of this post.
My focus here is on proton pump inhibitors because they remain the mainstay of treatment and are often prescribed as empiric therapy without further workup unless found to be ineffective. As a naturopathic doctor my goal is to treat the cause of disease whenever possible; palliative approaches like PPIs may help manage symptoms in the short term but do little to address the underlying problem. Due to the significant downstream effects of acid suppression on digestive function, immune function, and cognitive/neurological function, using proton pump inhibitors indefinitely is not my first choice – especially when there are many alternative methods available that help correct reflux.
