
Humans have eaten wheat for about 8000 years. But until recently (within the last 100 years or so), nearly all bread was made sourdough-style, with starter cultures rich in lactobacilli as well as some other bacteria and yeasts. These bacteria pre-digested most of the gluten protein for us.

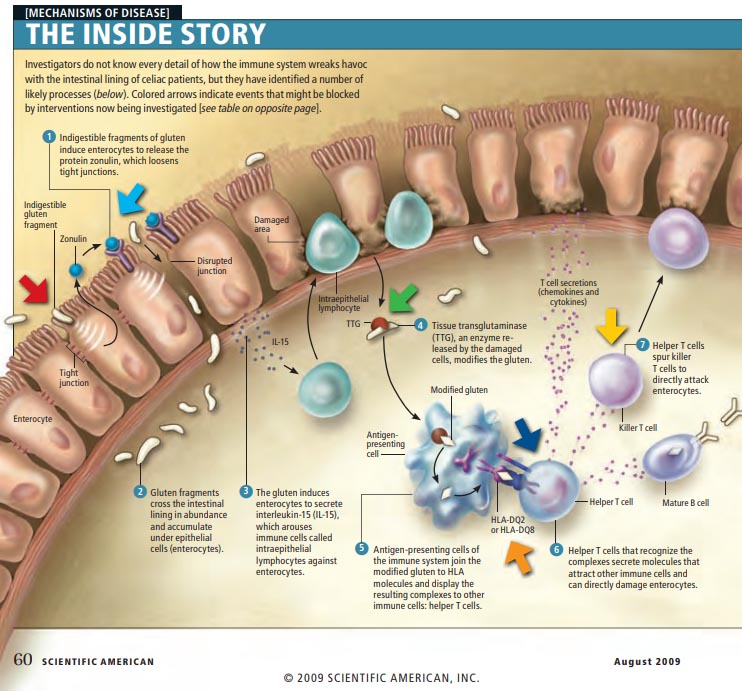
Our pancreatic enzymes digest proteins into small peptides or single amino acids. Gluten has a high content of the amino acid proline which puts many “kinks” in its structure and therefore prevents human digestive enzymes from cutting it into tiny pieces. The largest fragment of gluten left over is 33 amino acids long. There are at least 50 toxic fragments of gluten; these have been mapped to specific domains in α-gliadin: cytotoxic activity (aa 31-34), immunomodulatory activity (aa 57-89), zonulin release and gut-permeating activity (aa 111-130 and 151-170), and IL-8 release in celiac disease patients (aa 261-277).
The cells of the small intestine are knit together by tight junctions which create a strong barrier. Nutrients from food should only be absorbed through the cells, never between the cells. One action of undigested gluten fragments is to upregulate a messenger called  zonulin which disrupts tight junctions and creates intestinal permeability, which is sometimes referred to as a “leaky gut”. Once the intestinal barrier is broken, gluten and other proteins can cross between the cells and encounter the immune system. In celiac disease (as well as non-celiac gluten sensitivity), this sets off a chain reaction of inflammation which causes further damage.
zonulin which disrupts tight junctions and creates intestinal permeability, which is sometimes referred to as a “leaky gut”. Once the intestinal barrier is broken, gluten and other proteins can cross between the cells and encounter the immune system. In celiac disease (as well as non-celiac gluten sensitivity), this sets off a chain reaction of inflammation which causes further damage.
Celiac disease affects up to 2% of the population. Non-celiac gluten sensitivity (NCGS) may affect up to 20%. There are several tests that can help us determine whether someone reacts to gluten:
- genetic tests for HLA DQ2 and DQ8 (35% have one or both; 95% of celiac patients and 50% of NCGS patients)
- antibody tests against gluten (deamidated gluten peptide) or the enzyme tissue transglutaminase
- tests that quantify intestinal permeability: lactulose-mannitol test or level of zonulin activity
- upper endoscopy with biopsy of the small intestine to evaluate macroscopic and microscopic damage
However, the “gold standard” is to eliminate gluten-containing grains from the diet for a period of time and monitor symptoms for improvement. In a healthy person without celiac disease, the intestinal barrier can recover in a short period of time, typically 3 days to 3 weeks. More extensive damage can take much longer to heal – in the timeframe of several months to several years.
Some common symptoms of gluten intolerance include (there are more than 200):
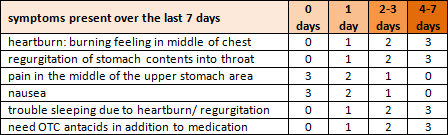
- digestive – abdominal cramps or pain, diarrhea or constipation, gas and bloating, nausea, reflux (heartburn), erosion of tooth enamel, frequent canker sores
- neurological – brain fog, ADHD-like behavior, depression or anxiety, headaches and migraines, numbness and tingling
- other – chronic fatigue, joint pain, fibromyalgia, eczema or other rashes, unexplained anemia, allergies and asthma
Grains that contain gluten: wheat, wheat derivatives (durum, semolina, spelt, farro, einkorn, kamut), rye, barley, triticale, malt [ https://celiac.org/live-gluten-free/glutenfreediet/sources-of-gluten/ ]
Common foods that contain gluten: breads, pastas, noodles, crackers, tortillas, baked goods, cereal, breakfast foods, sauces and condiments, breadcrumbs, beer, soy sauce, and many other processed foods!
Grains that do NOT contain gluten (but can become contaminated, so look for certified gluten-free versions): amaranth, buckwheat, corn, millet, oats, quinoa, rice, sorghum, teff
Most common foods that may “cross-react” with gluten according to a deranged immune system: potato, rice, oats, soy, millet, dairy, yeast (brewer’s and baker’s), milk chocolate, instant coffee
 My microbiology professor used to say that it takes 30 seconds of skin contact for triclosan to effectively kill bacteria. I don’t know about you, but I rarely see anyone wash their hands for that long — unless maybe they’re scrubbing for surgery. This means that we are flushing millions of gallons of triclosan-contaminated water (not to mention good money) down the drain for virtually no reason.
My microbiology professor used to say that it takes 30 seconds of skin contact for triclosan to effectively kill bacteria. I don’t know about you, but I rarely see anyone wash their hands for that long — unless maybe they’re scrubbing for surgery. This means that we are flushing millions of gallons of triclosan-contaminated water (not to mention good money) down the drain for virtually no reason.

